
“Before there are words, there is the wordless communication of the body.”
— Michael Changaris, Psy.D.
When early trauma is not addressed in therapy and remains untreated, it becomes deeply held at body level. This foundational dysregulation can cause severe somatic/medical symptoms for the young child and much later for the adult. There is a strong correlation between early child abuse and the development of autoimmune disorders thirty years later. See the Kaiser Ace study (1). Often, there is no language to address this type of trauma since it belongs to the pre-verbal realm. Therefore, different therapeutic modalities need to be put in place to see effective results.
Early trauma means in utero, birth and zero to three years. For some, it is up to 5 years and beyond. The earlier the trauma, the more likely it is to spread to a variety of systems (muscular, digestive, nervous), causing debilitating symptoms.
The missing piece that traditional and to some extent some somatic psychologies seem to miss lies in the regulation of the physiology. This is a necessary prerequisite to successfully renegotiate past and recent traumatic experiences. Somatic Experiencing has redefined how to support these clients with tools that involve building resiliency and self-regulation as a reliable foundation to come back to when disturbance occurs. Without this baseline, early trauma’s powerful dysregulated physiology has a tendency to overpower some of the best tools and techniques we have to down regulate the fragile nervous system, making them useless.
 Self-regulation
Self-regulation
In the physiological sense, this process is usually referred to as homeostasis. Self-regulation/homeostasis can be seen as one of the elements of resiliency, since it can be defined as the tendency of any system to return to equilibrium after something disturbs it. The idea of self-regulation/homeostasis presumes psychological or somatic capacity to maintain equilibrium and return to stability after disturbance. Of course, with individuals suffering from traumatic stress, such equilibrium is often no longer their tendency. Their tendency is more often toward disorganization and lack of stability. Instead of natural equilibrium, such individuals often have to exert tremendous effort – psychologically or physiologically – to manage their lack of stability. In other words, their capacity for self-regulation is inhibited. We can presume that this in turn decreases their overall resiliency (Kathy Kain) (2).
When the capacity for true self-regulation is restored, much less effort is expended to move to, and sustain, equilibrium. Energy is no longer consumed in the process of actively managing disequilibrium, but rather is available for other functions. This is where we see how critical self-regulation is in building resilience. When someone is able to self-regulate, there is less demand on both their psychological/emotional self, and their physiological/somatic self. That reduction in demand leads to greater resiliency. The client gains greater trust in her capacity to respond positively to life challenges, to re-establish equilibrium after such challenges, and to gain insight and strength from meeting those challenges. This is the very definition of a resilient client (Kathy Kain) (2).
Safety as pre-requisite
 Creating a safe haven, building trust, establishing reliability, holding a secure base for the child, managing closeness and distance, handling separation and distress securely are the bulk of a caregiver’s responsibilities. These are the key words that determine safety for a child (Steve Terrell) (3).
Creating a safe haven, building trust, establishing reliability, holding a secure base for the child, managing closeness and distance, handling separation and distress securely are the bulk of a caregiver’s responsibilities. These are the key words that determine safety for a child (Steve Terrell) (3).
Professor Stephen Porges (4) of the University of Maryland, U.S.A. uses the word neuroception to describe how neural circuits distinguish whether situations and people are safe, dangerous or life threatening. These are the filters put in place early on (our senses) that operate 24/7 to assess for safety. People and the environment are sorted out in the “safe” or “unsafe” categories. If safety is lacking, strategies are put in place in order to survive. Unfortunately, these strategies persist well beyond infancy into adulthood and survivor mechanisms continue to operate even though the threat is gone.
The autonomic nervous system
A little detour in defining the nervous system branches is necessary:
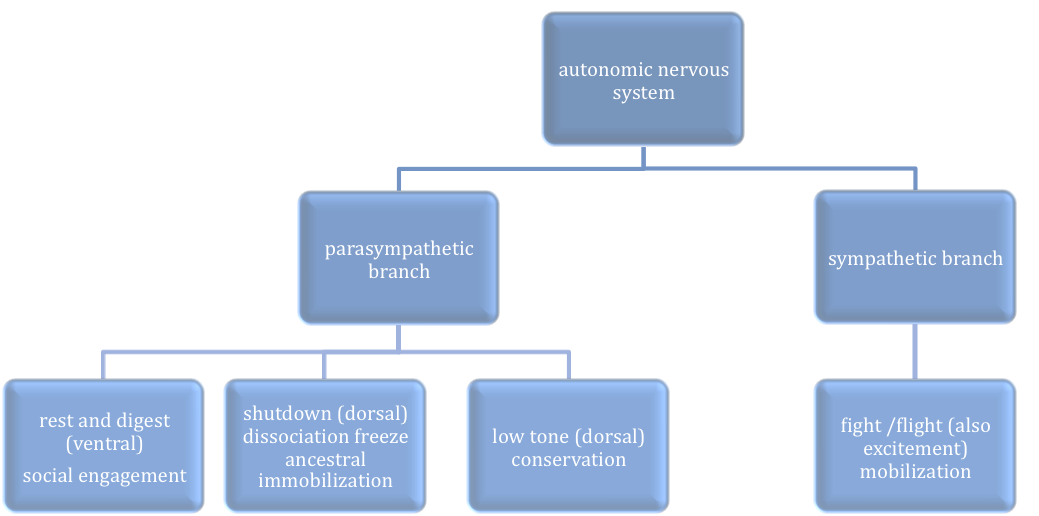
The Parasympathetic branch of the ANS has several sub-branches: the most restful state is what we call “ventral” (the belly side of the vagus nerve described in the polyvagal theory (4)) which means relaxation, settling, soothing and being able to relate. Kathy Kain calls it the low cost of doing business: we can digest, filter toxins and operate in a comfortable state while we do our “housecleaning” at a biological level. It is third in developing.
“Touch is the base of our sensory world; it is the first way we learn to relate with others and ourselves.”
— Michael Changaris, Psy.D.
Another sub-branch is the ancestral “reptilian” one that protects us by shutting down all necessary functions when overwhelmed. This is the state of freeze, dissociation, depression, numbness, slackness and immobility. We also call it “dorsal” as in “the back side” of the vagus nerve of the polyvagal theory (4). This is the high cost of doing business: there is no energy for biological functions since it is monopolized for survival. This is a highly conserving and protective state and biological processes come to a stop. Survival comes first by going limp under shock (like the opossum). It is first to develop.
The third sub-branch is called “low tone”, not so well known in the literature but a little gem in itself when the ventral is not accessible: this is a conserving state as well, but biological functions ARE happening and all energy is devoted to them. There is, in this state, no extra energy left for social engagement.
The Sympathetic side of the ANS is the one that keeps us on our toes: when there is danger, our fight/flight responses come into action. Biological functions are diminished: the system will choose to spend energy on an escape or a fight for survival rather than digesting or filtering toxins. It is also the system that provides some healthy arousal when we get happily excited. It is second to develop. When the Sympathetic system increases with high activation and a specific threshold is reached (different for everyone), the Parasympathetic system “brakes” the arousal. This is the equivalent of the emergency brake on a car. A shutdown occurs.
Both the sympathetic system –activation- and the ancestral parasympathetic system –shutdown- are on board at birth, but the branch of the parasympathetic system that enables us to rest and restore comes on board much later through co-regulation with the caregiver. It is easy to see that if this co-regulation does not happen because safety is missing, we might never develop this healthy soothing and comforting system. As we grow up, we learn to operate between high activation and complete shutdown, never having a chance to find the middle ground. The hallmark of early trauma is living between these two polarities.
Which brings us to attachment and the relational piece: when a baby needs to find safety with a caregiver (the one who responds the most fittingly to the baby’s needs and distress), and it is missing, the filtering system for safety is jeopardized towards the “unsafe”. The relational field is disrupted at a physiological level. The co-regulation that is supposed to happen with the caregiver in a safe environment fails. If there is no co-regulation, the baby does not learn to self-regulate and it persists into adult life. With a lack of safety, management strategies are put in place to stay alive, which will affect the baby and later the adult at relational (attachment) and social engagement level because both co-regulation and self-regulation were jeopardized early on.
Window of Tolerance

Living in the window of tolerance (blue) means riding the wave of activation and de-activation with our nervous system/physiology coming back to equilibrium relatively easily throughout life’s challenges. The system goes up and comes down almost naturally in a regulated way. As nervous system activation rises, we might leave the “blue layer” and enter the green zone. We use fantastic management techniques (#) to push our physiology back into the healthy blue zone. In fact, we are in a “faux window”, trying to manage the activation. We have become master over-riders of our own distressed physiology. These management techniques fool ourselves by thinking that we are back in the window of tolerance. We are not. This is not regulation, this is management. Example: C is challenged by social engagement and starts texting feverishly on her cell phone at the party to “down-regulate” her anxiety, isolating herself instead of connecting with other guests. This would fit the upper green zone of management techniques.) Sadly, many forms of electronics have become the (false) new regulators of distressed physiologies.
Sometimes, we get aroused by difficult and heartbreaking events (death of a parent, loss of a job, loss of a home, domestic abuse etc…) and we leave the green zone for the red one. Living in the high activation upper red zone can also become part of our daily grind as we “stay up” with high anxiety or high anger in the red zone permanently: this becomes a way of life. As we move closer to threshold the system gets overwhelmed and shuts down for protection. Living with depression means staying mostly in the lower red zone of shutdown. When we are in both these states of high activation or shutdown (red), we use coping mechanisms (*) to control symptoms and attempt to function. Example: B lives mostly in a state of high anxiety and has found ways to control his distress with obsessive thoughts and compulsive actions, which refers to an OCD diagnosis. Drugs (weed/alcohol/downers) aim at calming down a system in high distress (upper red zone). In a state of high shutdown (lower red zone), we might reach for “uppers” like cocaine or we might become promiscuous to feel alive and present although we have become numb and listless. I see coping mechanisms as somewhat more rigid and ingrained than management techniques.
These coping mechanisms come at a great price: as we use great energy to come back to the window of tolerance and manage our symptoms, our vitality is being hijacked and there is no energy left to live. This system exhausts itself very soon, taking a toll on the physical health and wellbeing.
There are, of course, healthier management techniques/coping mechanisms not mentioned here and effective medication to address these states. Some of the healthy tools to reach for could be: walk on the beach, sit by a tree, yoga, meditation, be with a pet, run, music, dance and many other art forms to name a few. Reaching out for a safe human being to regulate with seems to be the most effective in achieving parasympathetic soothing and staying in the blue zone.
This is a very rough graph that can’t possibly show the multitude of variations that a client can present. Developmental trauma exists between high activation and shutdown (red) and more often than not in the dorsal state of freeze (low red). For many, the sympathetic arousal system is used to function on a daily basis in order to avoid feeling the numbness of depression. This is what clients refer to as the “go-go-go” mode.
How table work helps
To address pre-verbal states and disrupted physiology, I use table work and touch therapy: they allow the client to stay somatically present, regulate physiological responses, and minimize the potential for being overwhelmed by strong physiological sensations (Kathy Kain). These table techniques are used as a resource for the client. This modality makes space to unload the traumatic stress physiology slowly. It accesses states of calm (the low tone state) that other modalities can’t. It is a gateway to re-establish regulation as a base to come back to when the early physiology has been disrupted. Table and touch work slowly get the client back within a healthy physiology.
Through healthy co-regulation with the therapist, new neuro-pathways are established and survivor behaviors can abate. The client gets to re-sort the world with a different lens: the lens of safety through co-regulation. Table work and touch therapy help establish a new basement, a new foundation: they help the client trust differently.
When regulation is established, the conditions are set to unpack the bigger and scarier stuff, the ghosts in the closet. What has been held at bay by management techniques will surface as the client regulates. Slowly, the resourced body will release some hidden stress responses. We process them as they come up.
Practically, here is a way we might want to start to resource a client. There are variants to this protocol and it is understood from the very beginning that my touch is non intrusive and respectful. Lying down on your back on the table or sitting up, I will hold your kidneys/adrenal region with the palm of my hand. When the kidneys are held safely, the body starts to relax, stopping the flow of Cortisol (stress hormone), telling the brain that it is possible to rest. We are imprinting new pathways and telling your system that you are safe, not alone and support is readily available. There is no need to cling to your survival strategies. This needs to be repeated many times, and slowly, regulation comes in.
Later, I might hold the brainstem if I see that it is telling your body that the environment is not safe. Your brainstem is your “control tower” scanning for dangers: the dangers from the past, not present in the therapy room. Depending on your needs, the hold could be ten to twenty minutes even longer. The result could be a felt sense of relaxation, some body sensations or some movements starting to form: each person has a different history and goes through her own process at a different pace. This is not a “relaxation” technique, this is repairing a bond, learning to co-regulate safely, learning to trust and establishing a solid base for more therapeutic work.
The gut is another important piece to hold in this protocol. It comes much later when enough regulation has come on board. There are many areas of your body that hold trauma and many others that we use as resources to re-establish healthy physiology. Gradually, as we work through the protocol, stress responses will bubble up and they will be attended to as we go.
Kathy Kain adds: “These techniques seem to target the most common patterns of hypervigilance and bracing in preparation for threat. By using direct contact with specific physical structures and regions of the body that play a large role in physiological resilience and self-regulation, the practitioner can invite their clients to alter long-standing habits in their stress responses. As clients are supported in letting go of these habitual patterns, they become more adept at allowing the full range of physiological responses to flow without the urge to stop or suppress them; they stay more somatically present, even in the face of strong somatic experiences”.
A last important note: as we work towards regulation and more settling, the purpose of this work is not to strip anyone of their healthy organic self-protective mechanisms. If they are onboard, they will be readily available when needed.
(1) https://www.cdc.gov/violenceprevention/acestudy/index.html
(2) Some of this material has been reprinted with author’s permission. See Kathy Kain’s Touching Trauma article. http://www.somaticpractice.net/
(3) http://www.austinattach.com/Home_Page.php
Quotes are from Michael Changaris’ book TOUCH: The Neurobiology of Health, Healing and Human Connection (Life Rhythm, 2015)